


Toxicological Flu, Cyanide and "Covid-19" [Abridged]

[P]ollution remains responsible for approximately 9 million deaths per year, corresponding to one in six deaths worldwide. ... [R]eductions in deaths from household air pollution and water pollution are offset by increased deaths attributable to ambient air pollution and toxic chemical pollution (ie, lead). Deaths from these modern pollution risk factors ... have risen by 7% since 2015 and by over 66% since 2000. [The Lancet, 2019]
…[H]ydrogen cyanide pollution from refineries is poisoning communities nationwide. Yet the EPA has failed to make these refineries clean up their act. [Earth Justice. May 14, 2019]
The most hazardous [cyanide] compound is hydrogen cyanide, which is a gas and kills by inhalation.[Wikipedia]
Cyanide prevents the cells of the body from using oxygen. [CDC]
Cyanide is naturally found in tobacco, and smokers can have more than 2.5 times the mean whole blood cyanide level of nonsmokers, though this is generally not enough to cause poisoning. [emedicinehealth]
Chronic exposures [to low levels of hydrogen cyanide] ... produced exposure-related symptoms including headache, weakness, and objectionable changes in taste and smell (El Ghawabi et al. 1975), but the authors failed to relate symptoms to air concentrations... [NIH]
Carbon monoxide is the most common cause of poisoning worldwide, often mistaken for a viral syndrome such as influenza. [Wikipedia, wording now modified keep everybody clueless]
... 60 percent of Americans are left breathing air dirty enough to send people to the emergency room, to shape how kids' lungs develop, and to kill... [Environmental News Service]
Abridged version
(This article is abridged from Part I of the original which covers other flu-like illnesses including West Nile Virus, Swine Flu, measles, SARS, and the 1918 Flu at length)
Overview
Flu and pneumonia symptoms induced by airborne pollutants are commonly mistaken for and medically misdiagnosed as a viral or bacterial syndrome. Medical training and research funding emphasizes viruses or other alleged pathogens and gives little if any attention to toxicology.
Historical precedents reveal that governments are willing to take advantage of the gullibility of the public and widespread fascination with viruses and contagion to cover for industrial malfeasance. When industrial pollutants sicken, maim and kill, blame is laid on a new virus and virus hunters are put to work to find it. Research with exclusive attention given to alleged "viral causation" is paid for by oversized government and industry grants.
Yet evidence of viruses is weak. Virology habitually ignores the scientific method, though it gives an appearance of being "scientific" through specialized jargon and technological complexity. If actual science were the aim it would require taking into account confounding factors, yet virologists ignore confounding toxicological factors at every step: they ignore causal relationships of toxic substances present in indoor and outdoor environments, in the laboratory experiments they perform, and in their so-called "virus stocks."
Due to the mind-numbing myopia generalized in academia and in the population, many obstacles must be overcome for a researcher or writer who wishes to bring into view anything outside the conceptual constraints of the virus/pathogen paradigm. Many objections arise spontaneously in those who are unable, even temporarily, to suspend disbelief in order to conceive of what may have been misinterpreted or overlooked—even when the truth is literally right before our noses.
Vehicle emissions and emissions from oil refineries are notorious for causing all kinds of illness, even death, and are especially associated with respiratory illness. The new practice of fracking has exponentially augmented already-potent toxic assailants from refineries and fuel burned in vehicles and indoor stoves and boilers. In particular, increases in hydrogen cyanide associated with fracking may be the cause of increased incidence of "new symptoms" attributed to Covid-19 like feeling unable to breath and changes in smell and taste. According to Earth Justice's 2019 report, though limits on hydrogen cyanide released into the atmosphere are set for specific refineries in the U.S., levels are not monitored by the Envirnomental Protection Agency save via monitoring of its so-called surrogate indicator carbon monoxide—levels of which do not correspond with hydrogen cyanide levels. Moreover, as it has been discovered that refineries are exceeding their stated emissions of hydrogen cyanide, they in turn have appealed for higher and higher limits. In the now over-industrialized regions of Asia and Latin America, industrial oversight is even more lax and the population less likely to pressure governments to constrain widespread pollution. In many such countries, vehicle emissions regulations are non-existent; people ignore horrendous pollution considering it a part of life in a continuum which younger generations perceive as having no beginning, no developments, and no end.
Medical tests for "viruses" also look for surrogates: proteins claimed to be part of a virus (in the case of PCR testing) or reactive to a virus (as in antibody tests). When a patient or asymptomatic person is said to be "positive," the illusion of a deadly viral illness is cemented on the consciousness of all. Yet, contrary to popular belief, "viral genomic sequences" that PCR tests are allegedly based on are never empirically found but contrived via complex computer assembly of thousands of tiny bits of protein codes of unknown origin and significance to conform to templates preselected from an international database of likewise never-empirically-found but arbitrarily constructed "viral genomes." When PCR finds increased amounts of select short amino acids in sick people, it does not confirm the presence of a virus, an entity that is only alleged to exist. The breakdown of cells during sickness leads to a greater amount of cellular debris—including amino acids that viruses are alleged to be made of—than during health, which can lead to a "positive" PCR test since proteins claimed to be part of viruses are found in all humans. Even large numbers of completely healthy people—along with papayas, goats, coca cola, sea water, etc.—will be "found positive" when a high number of PCR doubling-cycles is used, as has been commonplace in the Covid-era. They are then labeled “asymptomatic carriers.”
Likewise, proteins called "immunoglobulins" detected by "antibody" tests are naturally found in greater amounts in sick people as they are used by the body for binding and repair. They are not specific to "viruses" or even to disease: globulins are employed in recovery from any kind of injury and are found in especially large amounts in pregnant women as they are used to build the placenta (resulting in high numbers of "false positives" among pregnant women for so-called "HIV antibodies," for example). The fraud of so-called "antibody" testing has been exposed by German evolutionary biologist Stefan Lanka and by the Italian scientist Stefano Scoglio, among others.
https://www.drrobertyoung.com/post/dismantling-the-viral-theory
Toxicological Flu
Perhaps you've never heard of "toxicological flu." I certainly hadn't until I began to discover articles written on it by medical researcher Jim West.
West is the researcher responsible for reviving the buried 1950s work of Morton S. Biskind MD and Ralph R. Scobey MD on pesticides and polio. Perhaps less well-known are West's detailed articles showing association of various sources of toxic air pollution with flu-like illnesses including whooping cough, swine flu, West Nile Virus disease, SARS, measles, and more. One of the best introductions to the subject is his article on the so-called swine flu of 2009:
"Flu is nearly always considered viral, as evidenced by a search of CDC (Centers for Disease Control) website, the New York Times, or any media. Medical campaigns vaccinate millions worldwide, purporting to protect against flu epidemics, yet the symptoms of viral flu are the same as those of toxicological flu, and flu epidemiology makes toxicological sense.
West takes carbon monoxide poisoning as an example, since it's "well documented and commonplace," and cites Dolan et al (1985), who write:
"[T]he literature is well supplied with reports of patients with subacute CO poisoning who were misdiagnosed as having [virus] influenza and sent home with disastrous consequences."
The Great London Smog of 1952
In 1952, the UK government tried to cover up thousands of deaths from coal pollution by passing it off as a contagious influenza, only later admitting they'd "made a mistake." Meanwhile, they'd stealthily given the thick pall of smoke that had blanketed the city streets the misleading name "the Great London Fog." Smoke from "a million chimneys" of coal-burning open hearths had filled the air all winter. But during five days, temporary weather conditions pushed things to an extreme.

"To cover up the true extent of the smog disaster, the government invented a [viral] influenza epidemic. In fact research has shown there was no epidemic and that the thousands of people who continued to die for the next four months did so because of air pollution."
—Paul Brown, "50 years after the Great Smog, a new killer arises.”
Devra Davis, PhD, wrote an article on the 1952 public health disaster in History Today. She has documented many official air pollution many coverups in her book, When Smoke Ran Like Water: Tales of Environmental Deception and the Battle Against Pollution.
Though public pressure in the ensuing decade forced the UK government to enact policies to reduce pollution from coal, and coal used in indoors was gradually displaced by central heating, the reduction in thick, visible smog from coal was replaced by emissions from an ever-growing number of motor vehicles on the road.
Near constant media fear-mongering about deadly viruses has numbed the minds of the majority. These days, many people can hardly think in terms of anything else as being the cause of respiratory illness. When a bit of attention is given to other things that might cause or exacerbate illness, these are couched in politically-correct, career-safe terms as "cofactors" or "risk factors."
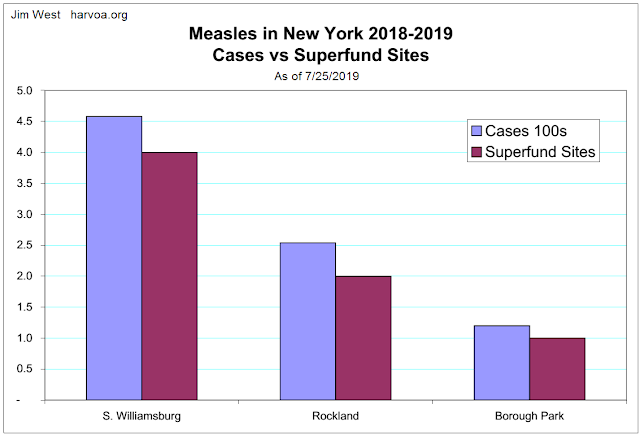
New York measles outbreaks, 2019
"The epidemics began late 2018 and continue to date (7/29/2019). It is possible that New York may complete a 12-month epidemic, which would be unusual because measles is supposedly a seasonal disease," West reported in 2019 in a detailed study.
"In the days leading to April 9, 2019, measles incidence spiked in the Brooklyn neighborhoods of Williamsburg and Borough Park," two of the three New York epicenters of the outbreaks, the third being East Ramapo in Rockland County. The Brooklyn outbreaks were blamed on the high concentration of ultra-Orthodox Jews in the area refusing to vaccinate their children, and Mayor Blasio ordered heavy fines for such families if they refused to meet a vaccination deadline.
In a study of 21 cities in China, Chen et al (2017) found "evidence that measles incidence is associated with exposure to ambient PM2.5."
Possible association with other kinds of pollution was not studied.
West identifies a number of new sources of contamination in the area of the Brooklyn epidemics:
A new power plant opens.
The use of toxic fracking gas fuel increases.
A new fracking pipeline opens.
EPA remediation disturbs Superfund site pollution.
Record-high petroleum production and export.
Modified refinery protocols may have been applied globally, related to fracking. High toxicity fracking fuel used in power plants increases outdoor air pollution. Used in stoves and boilers, it increases indoor pollution.
These were added to constant, old hazards:
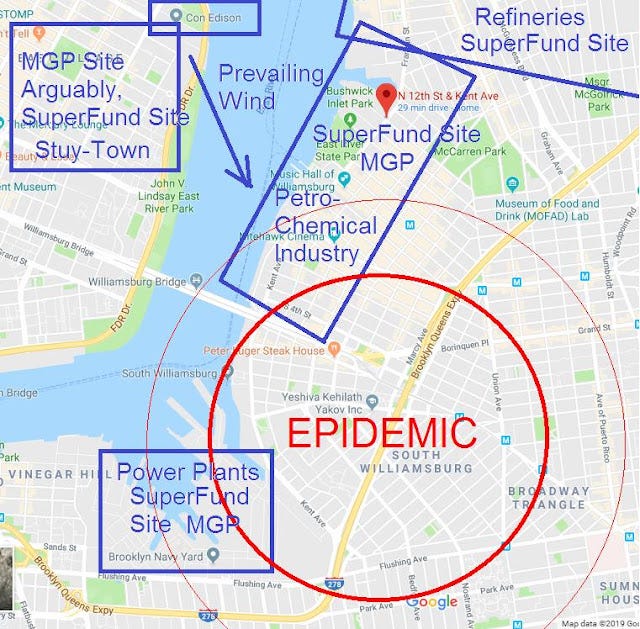
Power plants are near and upwind.
EPA Superfund sites indicate a legacy of poisoned earth and water, leading to indoor air pollution.
Manufactured Gas Plants (MGP), defunct, became Superfund sites.
Refineries, defunct, became Superfund sites
Superfund sites correlate with epidemic epicenters.
After much further detailed review, West concludes that pollution was the cause of the epidemics, but that industry stranglehold on all things health-related means that relevant data is never collected, studied or made available to the public:
With environmental factors avoided, virus causation is therefore MOOT (i.e., unresolved, debatable). The need for emergency vaccination must then be moot.
In 2020, something much more serious than the measly measles would hit New York. Yet New York epicenters of a "new illness" would be the same:
Williamsburg (Brooklyn, NY)
Borough Park (Brooklyn, NY)
East Ramapo (Rockland County, NY)
But first it will strike Wuhan, Milan, Madrid.
China pollution, an ongoing nightmare
The hazes can be choking and can reduce visibility at noon to a few tens of yards. Fumes belch from factory chimneys, coal-fired power plants, heating systems in apartment blocks, and millions of road vehicles. When the weather traps smog in the streets, city hospital admissions soar and the morgues fill.
— YaleEnvironment360 (2018)
Mark Hertsgaard writing for The Atlantic Monthly on Guangdong Province, where the greatest outbreak of SARS took place in 2003, says,
At least five of the cities with the worst air pollution in the world are in China. Sixty to 90 percent of the rainfall in Guangdong . . . is acid rain. . . people’s lungs and nervous systems are bombarded by an extraordinary volume and variety of deadly poisons. One of every four deaths in China is caused by lung disease.
—cited in Jim West, The SARS Epidemic: Are Viruses Taking the Rap for Industrial Poisons? (emphasis mine)
In many Chinese cities, pollution from sulphurous coal reminiscent of London circa 1952 is combined with choking exhaust from tens of thousands of motor vehicles.
"The unprecedented speed of industrialization and urbanization has combined two eras of pollution."
— How a ‘Toxic Cocktail’ Is Posing a Troubling Health Risk in China’s Cities, YaleEnvironment360

Overwhelmed with pollution, the country's largest cities like Beijing and Shanghai have implemented restrictions that have motivated polluting industries to relocate to lesser known parts of China, such as Wuhan.
Wuhan, December 2019
pneu·mo·nia | \ nu̇-ˈmō-nyə , nyu̇- \
: an acute disease that is marked by inflammation of lung tissue...
— Merriam-Webster
Wuhan is a city of over 11 million residents, China's seventh largest—a"China thoroughfare" located at a central crossroads of the densely populated mideastern part of the country. Called "the Chicago of China," it is among the most polluted cities in the entire world. A joint study published in the WHO bulletin lists Wuhan as one of a handful of Chinese cities with the worst levels of multiple contaminants.

In December of 2019, a number of patients interned in a Wuhan hospital were reported to have atypical pneumonia. In fact, this is not uncommon: 20-30 percent of pneumonia is generally tagged as "atypical." In a country of more than a billion people, and in a polluted city of millions, it is not unusual to find a significant number of people with pneumonia (both "typical" and "atypical") along with other lung conditions of some variety.
Growing social media concern in China throughout the month of December about a possible "new outbreak" centered in Wuhan at least partially reflected lingering fears concerning possible reemergence of a SARS-like respiratory virus after the highly dramatized 2003 epidemic. Given the chronic pollution and respiratory trouble plaguing China, these rumors may have been without real merit: social media is not known for objectivity. On the other hand, there may have been a very real new threat.
Pneumonia is designated atypical whenever tests have been done and the bacteria or other organisms typically blamed for causing the condition are not found. Often atypical pneumonias are blamed on other microorganisms, but the medical establishment's near-exclusive blaming of microorganisms for such conditions is disingenuous. Many if not all microorganisms that are claimed to be harmful pathogens are found in the sick and healthy alike.
Moreover, as Stefan Lanka has pointed out, noninfectious causes of pneumonia are often suppressed—doctors and the public kept in ignorance—even though they are described in the scientific literature:
There are actually several causes of atypical pneumonia which are not “infectious”...
Causes include the breathing in of poisonous fumes, solvents, and other chemical products...
He goes on to enumerate a number of other documented noninfectious causes of pneumonia.
Though Lanka mentions "poisonous fumes ... and other chemical products," for whatever reason he neglects to call attention to air pollution which often contains both of these, as well as harmful particulate matter.
Air pollution is of special concern in such highly polluted places as burgeoning Chinese cities; both poisonous fumes and particulate matter are a source of irritation and congestion of the lungs.
According to stoppneumonia.org:
Air pollution is the leading risk factor for death from pneumonia. An estimated 30% (749,200) of all pneumonia deaths in 2019 were attributable to air pollution according to the GBD. Of all causes of air pollution, it is particulate matter measuring less than 2.5 micrometers in diameter – less than a 30th of the diameter of a human hair – that causes the largest burden of disease. This “PM2.5” is emitted both outdoors and indoors, from vehicles, coal-burning power plants, industrial activities, waste burning, farming practices, and household cooking and heating using coal, charcoal, wood, agricultural residue, animal dung, and kerosene.
The article also asserts that:
The estimated 2.5 million pneumonia deaths that occurred in 2019 will rise massively in 2020 after COVID-19 deaths are included. No other infection causes so many deaths, according to the Global Burden of Disease (GBD).
When a team of virologists and epidemiologists from Beijing arrived in Wuhan on December 31, 2019 to provide support amidst the growing social media alarm, their analysis of the situation included no toxicological survey. As typical bacteria were not found in the pneumonia patients, they immediately set to work to find a virus. A month later, Fan Wu et al would publish one of the two seminal studies from Wuhan.
Fan Wu's team analysed a crude sample of bronchial-alluvial lavage fluid (BALF) from a single patient and came up with tens of millions of amino acid reads of unknown provenance. From these they created over a million contigs—longer sequences invented by computer pasting short reads together—and decided the longest contig consisting of around 30,000 nucleotide pairs belonged to a new SARS-like virus!
Did you notice anything strange about this process? Even centrifuged culture supernatant, gradient-density purified to the alleged density of viruses, contains billions of nucleic acid molecules, the vast majority of which can be found belonging to humans and ubiquitous bacteria. But Fan Wu et al. performed no centrifuging, no filtering, no purification, and yet they claimed to have "found" and described a new virus.
The hypothetical sequence the virologists' computers created would be entered into the world database, and ALL virologists claiming to sequence SARS-COV-2 or its morbidly terrifying "deadly variants" would use it for their template. PCR tests for the "virus" would test for nothing more than one or two very short snippets of the in silico sequence.
PCR test invented out of thin air, panic ensues
On January 1, 2020, researchers at Charité Hospital in Berlin including professors Corman and Drosten began developing a PCR assay (test) based on social media rumors from China of a respiratory disease outbreak and on suspicion that it could be caused by a new SARS-like virus. There were no patients or patient samples in Berlin, and not even a single official report from China. And there were as yet no invented, hypothetical sequences of an alleged new virus. When the first provisional sequences became available online on January 10 and 12, the Charité researchers immediately put them to use to further their ambitious enterprise in the absence still of samples or of any published study from China. The paper describing their RT-PCR test for detecting the “new coronavirus” would be submitted to EcoSurveillance on January 21 and published within 48 hours of submission, failing to disclose the researchers’ conflicts of interest. In the meantime, before even superficial review or publication, on 21 January the WHO would recommend the Charité test for use everywhere. It became the most prominently used PCR test in the world for the alleged new virus. This was days before the first official studies from China were published on January 24 and February 3, 2020, both of which could not make the claim that they had shown the existence of a new virus causative of illness.
The fact that the World Health Organization (WHO) recommended the PCR test developed by Professor Drosten for proving the new virus, even before the publication of the two Chinese sequencing suggestions, is proven. Professor Drosten used unproven scientific data for his quickly globalised PCR-test for the 2019-nCoV, which was renamed with his participation SARS-CoV-2 on 07/02/2020. [i.e. Feb 7, 2020]
With the renaming of the description of a mere suspicion of a possibly defective or harmless virus “nCoV” to a dangerous pathogen “SARS-CoV-2” the impression was implanted in the public, that an actual SARS-virus was discovered in China, which causes a dangerous disease, namely SARS [Sudden Accute Respiratory Syndrome] ...
—Dr Stefan Lanka, The Misinterpretation of Viruses Part 2. (References omitted.)
Lombardy, Italy 2020
On January 31, 2020, a mere 10 days after the WHO's recommendation of the Corman-Drosten PCR test, the Italian Council of Ministers declared a 6-month national emergency after two Chinese tourists traveling from Wuhan "tested positive." That is, emergency state powers were declared a full three weeks before the first Italian citizen "tested positive" on February 20—a seventy-eight year old retired brick layer from the village of Vo' Euganio, who later died in the hospital while under hospital treatment for pneumonia.
The following excerpt is taken from an exceptional article detailing the many circumstances that would lead to overcrowding of several hospitals in the north of Italy in March of 2020. Note the mention of weather conditions aggravating the effects of pervasive pollution.
The Po River Valley in Northern Italy is cited as having the worst air quality in all of Europe. The air quality in the region has been deteriorating for many years. The cities in the Po River Valley are cited as having the highest mortality burdens associated with air pollution in all of Europe.
Along with the sheer volume of pollutants, the Po River Valley is known for its unique characteristics of low winds and prolonged episodes of climatic inversions turning it into a holding tank for atmospheric pollution.
The Lancet Planetary Health report from January 2021 estimated death rates associated with fine particulate matter and nitrogen dioxide pollution in 1000 European cities. Brescia and Bergamo in the Lombardy region held the morbid distinction of having the highest death rate from fine particulate matter in Europe. Two other Northern Italian cities, Vicenza and Saronno placed fourth and eighth respectively, in the list of top ten cities in this category. These locations correspond precisely with the highest incidents of upper respiratory infections occurring in Northern Italy as reported in the official pandemic narrative.
Ongoing and accelerating “epidemics” of idiopathic pulmonary fibrosis, (a severe and progressive lung disease), interstitial lung disease and high rates of bronchial and lung cancer were signature epidemiological features of Northern Italy long before an alleged virus ventured onto the scene.
—Michael Bryant, Italy 2020: Inside COVID’s ‘Ground Zero’ In Europe
The article also details the little-told fact that due to cuts in funding, the number of hospital beds has been gradually reduced for years in northern Italy and other places around the world, leading to overcrowding:
The net effect of these radical cuts to hospital infrastructure and services in the context of the covid hysteria were predictable; for years Italian ICU physicians have been reporting that flu outbreaks cause ICU units to fill up as was the case in locations across the world.
U.S. epicenters
Spikes in pollution caused by a federal relaxation of air quality standards in March [2020] led to increases in Covid-19 deaths in the most industrialized areas of the United States, new research suggests. Meanwhile, several other recent studies reveal that people who live in the most polluted areas ... are more likely to suffer severe symptoms and die from the disease.
The revelations, which many scientists have been expecting since air pollution is known to exacerbate respiratory diseases ... come as the White House is working to roll back numerous clean-air regulations, and as air pollution—which was declining for decades—is surging back.
—"A Surprise Surge in Air Pollution..." Elemental 7/19/20

The two largest US epicenters, the Tri-State Region [NY, NJ, CT] and Louisiana, are both amidst the largest petrochemical regions in the U.S., and downwind from power plants fueled by fracked-fuel.
— Jim West, Covid-19: Seeking the Environmental Trigger (2020)
West notes also that New York and New Jersey are also the sites of repeated earth spills "accumulated from centuries of unregulated industry." This contamination represents a constant menace to the health of the population, and is a likely contributor to epidemics:
Usually, epidemics in the US begin in, and are heaviest in, the New York City region, e.g., the 1916 polio, 1918 Spanish flu, The Great Polio Epidemic, West Nile virus, H1N1 flu, measles, and now, COVID-19. The cover story for each epidemic is a virus.
Chronic Air Pollution, New Dangers
West suggests chronic respiratory damage from air pollution in "Covid-19" epicenters was exacerbated by increases in pollutants associated with fracking, particularly increases in hydrogen cyanide—this, coupled with decisions to allow more of these pollutants into the atmosphere:
Postulate (pandemic trigger)
The pandemic trigger was a global decision to allow refineries to release higher levels of cyanide into the atmosphere and into the natural gas fuel stream. Cyanide is normally emitted from refinery converters ("crackers"), because converters generate cyanide from nitrogen compounds present in the oil. However, fracked oil can contain 20x higher levels of nitrogen compounds, and thus the necessity to dump cyanide into the atmosphere and fuel stream is pertinent to fracked oil [...] Unmarketable toxic waste accumulates and must be disposed.
—Covid-19: Seeking the Environmental Trigger by Jim West (2020)
(See the article for a more detailed explanation of fracking.)
He provides a table revealing correlation of production or import of fracked fuel with "Covid-19" epicenters:

Although death data is limited to the end of April/beginning of May of 2020, all the initial major peaks in deaths had occurred (or were occurring) by that time. Moreover, this does not affect the correspondence with pollution.
The high number of deaths shown for Wuhan (635.6 per 100,000 pop.) are based on West's assumption that deaths in Wuhan did not come to an abrupt end as China claimed.
China’s claim of low numbers occurred after it kicked out Western journalists. Yet, Western journalists choose to believe or disbelieve China’s statistics, depending on the agenda the Western medicos are pushing. For example, they disbelieve China’s numbers, as they hype the hazards of the COVID-19 virus, or want to accuse China for starting the epidemic, and they believe China’s numbers, as they point to China’s “successful” lockdown policy.
— Jim West, Covid-19: Seeking the Environmental Trigger
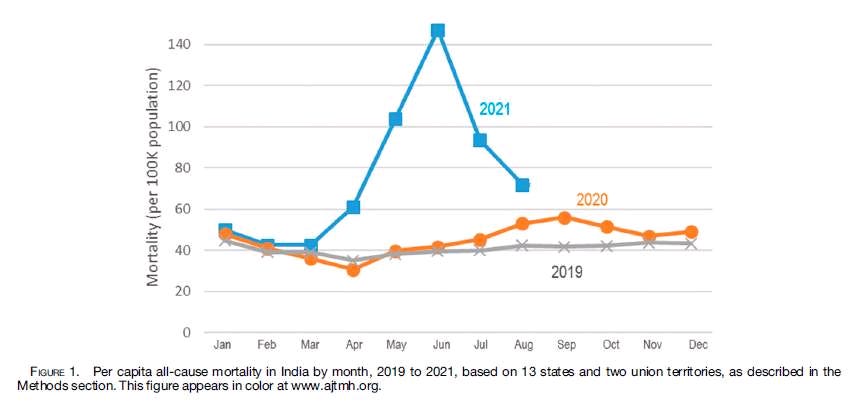
However, West’s assertion that the “pollution thesis would expect Wuhan COVID-19 deaths to be high and continuous” may be inaccurate. All-cause mortality (ACM) throughout the rest of the world shows spikes during specific weeks for specific geographic locations, the first wave of these beginning after WHO director Tedros declared a pandemic on March 11, 2020 (see ACM studies by Rancourt, et al.). The decline in excess deaths is generally as rapid as their rise. Thus another explanation should be sought. Is it possible that refineries emitted high amounts of pollution over relatively short time periods? Or could the rapid decline in excess deaths be due to the dry tinder effect (vulnerable people died off and those who remained were more resilient)? Or other variables such as drug overdosing entering into the picture? A combination of all of the above?
Similarities between "Covid-19", SARS, and the 1918 Flu
One of the major symptoms reported as being unique to Covid-19 is extreme hypoxia (deficiency of oxygen reaching the tissues of the body) manifesting in cyanosis—bluish or purplish discoloration, often seen in the lips or cheeks, due to deficient oxygenation of the blood.
Cyanide is one possible assailant that can lead to cyanosis, it's not the only one. It’s quite possible that others of the many deadly poisons in fracked fuel could have similar effects, and some kinds of RF radiation including 5G has been said to make oxygen unavailable to the body, as well.
Nor is this the first time cyanosis has been seen in a respiratory pandemic. Cyanosis may have occasionally been seen in SARS patients. But going back even farther, it was definitely part the 1918 Flu.
By the way, no "virus" was found or even looked for during the 1918 Flu. The concept of "virus" was very different in those days and constantly shifting with each passing decade, but more importantly the medical establishment at the time was convinced the flu was caused by a bacterium. Experiments were performed in Boston and San Francisco in attempt to show transmission by exposing healthy young male volunteers to army patients bedridden in hospitals with the flu, as well as attempting to infect the volunteers via phlegm or various bacterial cultures using every method they could come up with. All the experiments failed. None of the volunteers got the flu.
Several modern papers, including a study involving Anthony Fauci in the early 2000s, suggest the 1918 Flu was actually bacterial pneumonia. But again, finding a bacterium is no proof that it causes illness, as the authors of the Boston and San Francisco experiments demonstrated to their own bewilderment.
Morbidity and mortality in the "Covid Era": a web of crimes
“In all epidemics, the so-called epidemic disease is but one among several symptom complexes presented by the sick.”
—Herbert Shelton ND DC
COVID-19 and other morbidity/mortality is high at the epicenters. This all-cause increase is the actual pandemic and it includes children.
—Jim West, Covid-19: Seeking the Environmental Trigger (2020)
Moreso than with any past epidemic, 24/7 media alarm focused the attention of the entire world on a single threat (a novel coronavirus) and a single disease ("Covid-19"). Yet contrary to the conjured perception of epidemics of specific diseases caused by specific pathogens, the reality is quite different in any era. Particularly in the "Covid-era"—by virtue of multiple factors contributing to morbidity, broad diagnostic criteria, politically and financially-incentivized diagnostic bias and extremely corrupt handling—the picture is complex. Not only can pollution itself result in a wide array of syndromes ranging from measles to pneumonia to depression, heart attack or stroke, but other assaults including social and economic privation; medical/pharmaceutical "mistakes" or malpractice; and psychological effects of extreme media fearmongering, societal disruption, and forced masking and social distancing were added to the mix.
WHO and state-recommended intubation for "Covid" patients—in spite of early indications from China of the unnecessary harm caused by it—led to an 80% death rate among intubated patients worldwide—some suggest even higher. As brought to light in the article on Italy cited earlier:
Employing ventilators involves sedating the patient and placing a tube into the throat. Drugs such as midazolam, morphine sulfate and propofol are used in accompaniment with this procedure; drugs that come with contra-indications and warnings of side effects including respiratory depression and respiratory arrest. Midazolam and propofol are two drugs that are regularly used for assisted suicide and to put down death row inmates.
Midazolam in particular, an injectable anti-anxiety drug, played a prominent role in the UK where it was administered in lethal doses under the pretext of keeping care home interns from being over-anxious about the pandemic. The high number of deaths in care homes in spring of 2020 can be directly attributed to state-recommended drug overdosing of the elderly and the physically or mentally handicapped coupled with "do-not-resucitate" forms pushed by the establishment.
Similar policies in other countries led to increased deaths in nursing homes early on. Lockdowns led to unemployment, hunger and increased levels of depression and suicides, particularly among young males in cultures where they're expected to be independent and not fall back on family.
Post-vaccine rollout, various studies by Rancourt et al. show correlation of large waves of excess all cause mortality with vaccination campaigns in the United States, Australia, India and Israel—especially campaigns targeting poor and "at risk" populations. The horrific effects of the experimental "COVID" vaccines were not limited to those countries.
What West does that few others have attempted is identify a plausible environmental trigger that could have been what set things in motion. In this author's opinion, he's the only one who's given an adequate, plausible explanation for increased incidence of certain specific symptoms associated with "Covid-19," shedding light on symptoms myself and others I've interviewed personally (who didn’t visit hospitals or use prescribed medications) have experienced.
West also states that although 5G rollout has been suggested by some as the cause of a new respiratory pandemic, "This is unlikely because 5G protocol was not substantially present in all the epicenters, and the 60GHz frequency, the form of 5G that would purportedly cause COVID-19 symptoms, was not yet deployed. 5G is not a common denominator."
West does not deny the ability of electromagnetic radiation to exacerbate the situation, and later adds a section titled "EMF co-factor trigger for COVID" in which he describes how New York legislated invasive, ubiquitous installment of "smart" smoke detectors prior to the pandemic. He also tells of the following story of what appears to be the combined effect of pollution and EMF:
In another EMF instance, I interviewed a person with COVID-like respiratory disease where she was obviously suffering from high air pollution, as I too could feel its severity. I visited her apartment and found her sleeping quarter near Internet WiFi modem/router, with cables running near and many wall warts. Getting her to unplug all that brought instant relief from insomnia and clear progress towards diminishing COVID pneumonia symptoms.
With regard to deaths caused by drugs and ventilators, West remarks:
These deaths would not be an initial trigger for the pandemic, but rather an expansion and dramatization of the epidemic already prepared by chronic air pollution, then triggered by a severe increase in air pollution.
If you have questions related to this article, check out the long version or leave a comment below.
Toxicological Flu, Cyanide and "Covid-19"

And the Historic and Ongoing Manipulation of Public Perception (Unabridged)
Tobin Owl is an independent researcher/writer. Over the past three years he’s conducted in-depth investigation focusing on the history of modern medicine, medical science and the environment. The bulk of his articles can be found on his website, cryfortheearth.mystrikingly.com